How to Last Longer in Bed Naturally: The Complete Science-Based Training System to End Premature Ejaculation
Premature Ejaculation Causes: The Complete Scientific Guide
Introduction
Why does climax arrive sooner than you planned—sometimes almost the moment arousal spikes? If you've asked yourself this, you're not alone. "Premature ejaculation causes" isn't just a search phrase—it's a real, everyday question men ask in the privacy of their browser when worry, frustration, or relationship tension start to build. The goal of this page is simple: to replace guesswork with science you can trust.
Ejaculation is not random; it's a fast, hardwired reflex coordinated by the spinal cord and shaped by brain chemistry, hormones, and the balance between the sympathetic ("accelerator") and parasympathetic ("brake") nervous systems. When that balance tilts—because of penile hypersensitivity, pelvic floor over-activity, low serotonin signaling, stress, or specific relationship dynamics—the reflex can fire earlier than desired. Understanding these mechanisms matters, because each pattern points to different levers you can adjust.
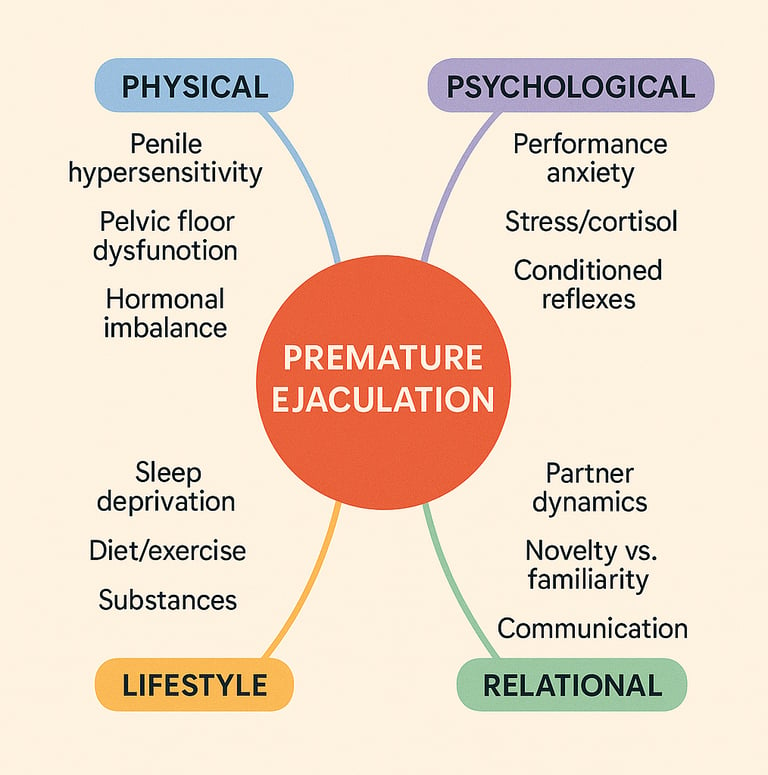
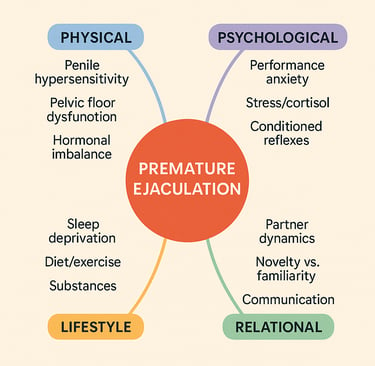
In this complete scientific guide, we'll translate neurophysiology into plain English, show how body, mind, and context interact, and organize the evidence into clear categories: physical, psychological, relational/situational, age and lifestyle. We'll also clarify when to seek medical input and how a cause-first map leads to smarter treatment choices. By the end, you'll understand premature ejaculation causes deeply enough to discuss them confidently—and to act with purpose.
Understanding the Ejaculatory Reflex
Neurophysiology Simplified
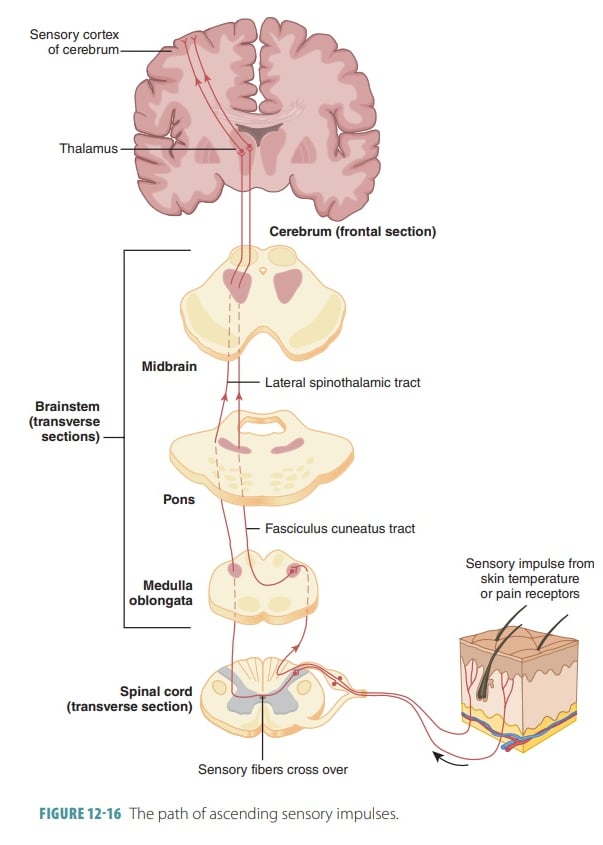
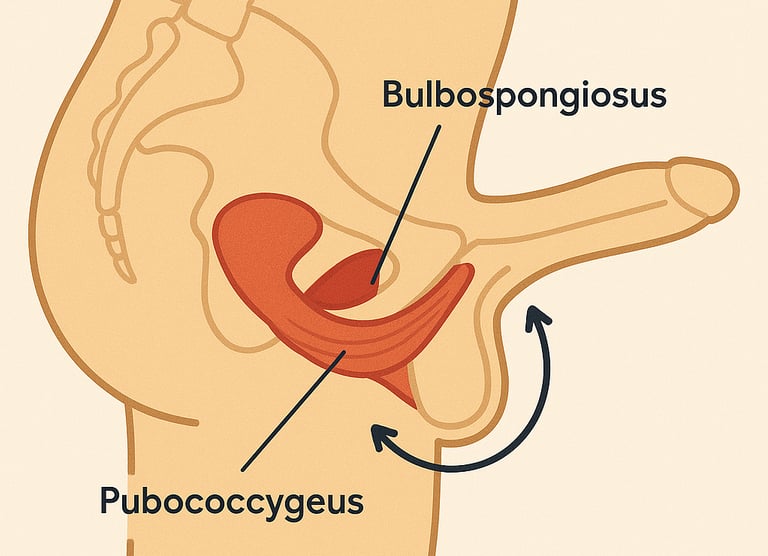
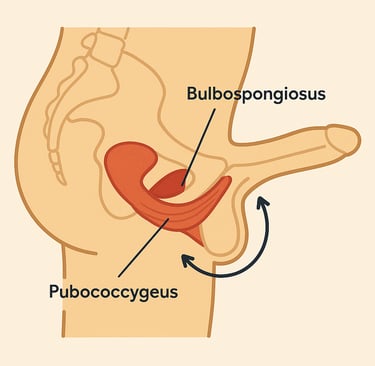
Close your eyes for a moment and picture this: your body has a hidden control room deep in your spinal cord. When sexual stimulation reaches a certain threshold, this control room receives urgent signals from thousands of nerve endings in your penis. These signals race up through the pudendal nerve, arrive at the sacral spinal cord, and trigger a cascade of automatic responses. Your breathing quickens. Your heart pounds. Muscles you can't consciously control—the bulbospongiosus and ischiocavernosus—suddenly contract in rhythmic waves, propelling semen outward.
This is ejaculation: not simply a matter of willpower, but a finely coordinated reflex that involves multiple neural circuits working in perfect synchrony.
The reflex unfolds in two distinct phases. During emission, the sympathetic nervous system takes charge, moving sperm and seminal fluid into the urethral bulb. Then comes expulsion, when rhythmic contractions of the pelvic floor muscles propel everything outward. The entire sequence is orchestrated by neurotransmitters—chemical messengers that determine how quickly or slowly the reflex fires.
Serotonin (5-HT) is the master brake. Studies published in The Journal of Sexual Medicine show that reduced serotonin activity, especially in the 5-HT2C and 5-HT1B receptor pathways, correlates with shorter ejaculatory latency times. Men with naturally lower serotonin levels or reduced receptor sensitivity reach the point of no return faster—not because they lack discipline, but because their neural brake system is less responsive.
Dopamine acts as the accelerator, heightening arousal and sensitivity. Oxytocin modulates post-orgasmic satisfaction and recovery. This neurochemical ballet explains why premature ejaculation often reflects an overactive reflex arc, hyper-excitability of the spinal centers, or an imbalance in these neurotransmitters—rather than "psychological weakness."
Think of it this way: if your body's ejaculatory control were a car, the spinal cord is the engine, neurotransmitters are the fuel mixture, and your conscious mind is the driver. When the fuel mixture is off—too much dopamine, too little serotonin—even the most skilled driver struggles to maintain control
Sympathetic vs. Parasympathetic Systems
Your autonomic nervous system operates like two opposing forces locked in constant negotiation. The sympathetic system—your body's fight-or-flight response—initiates emission and intensifies arousal. When activated, it floods your body with adrenaline, speeds up your heart rate, and pushes you toward ejaculation.
The parasympathetic system, by contrast, is your body's rest-and-digest mode. It allows relaxation, maintains erection, and extends the window of control. When these two systems are balanced, you can ride the wave of pleasure without crashing over the edge too soon.
But when chronic stress, anxiety, or overstimulation trigger persistent sympathetic dominance, the ejaculatory threshold drops dramatically. This "neural overspeeding" is a core mechanism behind premature ejaculation. Your body remains locked in high gear, unable to downshift into the calmer state needed for prolonged control.
Imagine trying to drive through a peaceful neighborhood while your car is stuck in racing mode—every slight acceleration sends you flying forward. That's what happens when your sympathetic system dominates: even minimal stimulation triggers maximum response.
Conversely, a well-balanced autonomic system—often achieved through pelvic floor retraining, breathing regulation, and cognitive relaxation—helps delay reflex firing. This physiological model explains why lasting improvement requires systemic rebalancing, not just behavioral tricks.
→ Understanding your nervous system is the first step. Retraining it is the solution
Teaches you exactly how to restore this balance through progressive neurological conditioning.
Physical Causes of Premature Ejaculation
Penile Hypersensitivity
Picture every touch, every sensation amplified tenfold. For men with penile hypersensitivity, the glans and frenulum are loaded with overactive sensory receptors that send rapid volleys of signals to the spinal ejaculation center. It's like having the volume dial on your nerve endings turned up to maximum—what should be pleasurable stimulation becomes an overwhelming flood of input that shortens latency dramatically.
This hypersensitivity can be congenital (present from birth) or acquired through local inflammation like balanitis or chronic irritation. Some studies suggest that circumcision status and glans exposure can modulate sensitivity, though evidence remains mixed. What's clear is that when your sensory threshold is too low, even gentle stimulation can trigger the ejaculatory reflex before you're ready.
Desensitization creams address symptoms temporarily by numbing nerve endings, but they don't retrain the underlying neural reactivity. True mastery comes from teaching your nervous system to tolerate higher levels of stimulation without reflexively ejaculating—a skill you can develop through progressive exposure and mindful attention training.
Pelvic Floor Dysfunction
Your pelvic floor muscles—especially the bulbocavernosus and pubococcygeus—play a dual role: maintaining erection and controlling ejaculation. When functioning optimally, they act like a sophisticated hydraulic system, regulating pressure and timing with precision.
But when chronically tense or hypertonic (over-contracted), they compress the urethra and overstimulate reflex pathways, leading to premature contractions. It's like having a spring wound too tight—the slightest trigger causes it to snap.
EMG-based studies show men with PE often display elevated baseline muscle activity. Their pelvic floor never truly relaxes, creating constant tension that makes the ejaculatory reflex hair-trigger sensitive.
The solution isn't just strengthening these muscles (though that helps), but learning to consciously contract and relax them. Pelvic physiotherapy and neuromuscular relaxation—including reverse Kegels and breathing exercises—can restore voluntary control and extend latency naturally.
Think of your pelvic floor as an orchestra: every instrument must play in harmony. When the strings are too tight or the drums too aggressive, the entire performance falls apart. Rebalancing this internal orchestra is fundamental to lasting control.
Hormonal Factors (Serotonin, Testosterone, Thyroid)
Your hormones and neurotransmitters interact in an intricate dance that determines ejaculatory timing. Here's what the research reveals:
Low serotonin levels increase excitability of the ejaculation center. Men with genetic variations affecting serotonin transporters or receptor sensitivity may have a naturally shorter latency period. This isn't a character flaw—it's biochemistry.
High testosterone enhances libido and sensitivity but may shorten latency in some men. It's the difference between a sports car (powerful, responsive, but requiring careful handling) and a sedan (steady, predictable). Neither is wrong, but the sports car demands more skilled control.
Thyroid dysfunction, particularly hyperthyroidism, has been directly linked to PE in multiple studies. When your thyroid produces too much hormone, it speeds up your entire metabolism—including your sexual reflexes. Correcting thyroid imbalance often resolves symptoms completely, highlighting the importance of hormonal screening.
Other hormones— prolactin and oxytocin—modulate post-orgasmic satisfaction and recovery. When this biochemical web is out of balance, no amount of willpower alone can compensate.
The biochemical foundation matters. If hormonal imbalances are sabotaging your control, the [Complete Ejaculation Mastery Program](https://how-to-last-longer-in-bed.com) helps you identify warning signs and guides you toward the right medical screening—while simultaneously training the neural pathways that work regardless of your starting biochemistry.
Psychological Causes
The Performance Anxiety Cycle
Imagine this scenario: You're about to be intimate. Instead of anticipation, your mind floods with worry. What if I can't last? What if I disappoint her again? What if this happens like last time?
Your heart rate spikes. Adrenaline surges. Your sympathetic nervous system—your body's panic button—activates fully. The very fear of losing control becomes the catalyst that causes it.
This is the performance anxiety cycle, one of the most self-reinforcing causes of PE:
1. Anticipation of failure → Tension builds before intimacy even begins
2. Increased heart rate → Reduced parasympathetic (calming) activity
3. Accelerated reflex → Rapid climax confirms your worst fear
4. Reinforced belief → Next time, anxiety starts even earlier
It's a vicious spiral where anxiety creates the outcome you feared, which generates more anxiety. Many men describe feeling like passengers in their own body—watching helplessly as the ejaculatory reflex hijacks control.
But here's the crucial insight: anxiety is physiological, not purely mental. You're not weak-willed or inadequate. Your nervous system has learned a maladaptive response pattern that can be unlearned through systematic retraining.
Breaking this loop requires understanding that anxiety triggers measurable changes: elevated cortisol, increased sympathetic tone, heightened nerve sensitivity. Address these physiological responses through breathing, progressive muscle relaxation, and exposure desensitization, and the psychological weight lifts naturally.
Stress and Cortisol Impact
Picture cortisol as the volume knob on your body's stress response. When life keeps that knob cranked up—work pressure, financial worry, relationship tension—cortisol floods your system day after day.
Chronic stress elevates cortisol, your body's primary stress hormone. Elevated cortisol dampens serotonin synthesis (remember: serotonin is your natural brake) and alters nitric oxide pathways crucial for sexual function. Over time, this biochemical shift increases ejaculatory urgency and reduces endurance.
Clinical studies (e.g., Psychoneuroendocrinology, 2019) demonstrate that men under sustained work or relationship stress report up to 40% shorter IELTs (Intravaginal Ejaculatory Latency Times). This isn't "in your head"—it's neuroendocrine reality.
The mechanism works like this: Chronic cortisol elevation → Reduced serotonin production → Lower inhibition of ejaculatory reflex → Faster climax. Your body remains in perpetual fight-or-flight mode, making calm, controlled arousal nearly impossible.
Stress management isn't "psychological fluff"—it's direct neuroendocrine therapy. Every minute you spend in meditation, every deep breath you take before intimacy, every stressor you address actively rebuilds the neurochemical foundation for lasting control.
Early Sexual Experiences and Conditioning
Your sexual reflexes are conditioned behaviors shaped by early experiences. For many men, early masturbation was done quickly—often in secrecy, rushed to avoid discovery by parents or roommates. You learned to reach orgasm fast, to finish before anyone noticed.
This repeated "rush pattern" becomes neurologically encoded. Your nervous system learns: Sexual arousal = immediate ejaculation. Later, during partnered sex, your body still follows this rapid, conditioned reflex—even when you consciously want to slow down.
This isn't permanent damage; it's learned behavior. And anything learned can be unlearned.
Think of it like learning to type incorrectly. If you practiced typing with wrong finger positions for years, those neural pathways become automatic. Relearning proper technique requires patience, conscious practice, and repetition. The same applies here: you're not broken, you're just running old programming that needs updating.
Reprogramming this pattern requires awareness and gradual retraining through techniques like mindful masturbation, stop-start exercises, and progressive exposure. Behavioral and mindfulness-based therapies target this core cause effectively—not by suppressing the reflex, but by teaching your nervous system a new, more adaptive response.
→ If conditioned reflexes are driving your PE, you need a progressive reconditioning system. The 4-Level Training Program guides you through exactly this process: from recognizing old patterns (Level 1) to installing new neural pathways (Levels 2-4) that give you conscious control.
Relationship and Situational Factors
Partner Dynamics
Close your eyes and picture two scenarios:
Scenario A: Your partner greets every pause with patience, every stumble with encouragement. She tells you, "Take your time, I love being close to you." When you need to stop, she kisses your neck, whispers reassurance, helps you breathe.
Scenario B: Your partner's face tightens with frustration when you ejaculate early. She sighs, rolls over, makes comments about "other guys" or "how it used to be." Every intimate moment carries the weight of unspoken judgment.
Which scenario makes control easier?
Emotional intimacy, communication, and partner understanding dramatically affect ejaculatory control. If a partner is perceived as judgmental, distant, or impatient, anxiety levels skyrocket. Your sympathetic nervous system activates, cortisol spikes, and the ejaculatory reflex accelerates.
Conversely, supportive partners help reduce pressure, fostering relaxation and slower buildup. Couples therapy often reveals that PE is less about one partner's physiology and more about the relational system—the emotional dance both partners perform.
Research shows that when partners actively participate in treatment—learning stop-start techniques together, creating non-judgmental spaces for practice—success rates double or triple compared to individual treatment alone.
Your partner isn't the problem, but the dynamic between you matters immensely. Open communication transforms PE from a shameful secret into a shared challenge you tackle together.
Novelty vs. Familiarity (The Coolidge Effect)
There's a well-documented phenomenon in sexual science called the Coolidge effect: novelty heightens arousal dramatically. New partners, new settings, new fantasies activate dopaminergic reward circuits in your brain, flooding you with excitement—and potentially accelerating ejaculation.
It's why first-time encounters or particularly exciting situations often trigger faster climax. Your brain's reward system is firing on all cylinders, overriding your conscious control efforts.
Overfamiliarity, on the other hand, may reduce stimulation and naturally delay orgasm. Long-term partners often report that while initial encounters were rushed, intimacy became more controlled over time as novelty wore off.
Neither is inherently good or bad—they're just different contexts requiring different management strategies. Understanding that situational context (new partner, exciting setting, or intense fantasy) plays a measurable role in ejaculatory latency helps you anticipate challenges and apply appropriate techniques.
The key insight: context isn't destiny. You can learn to maintain control even in highly novel, exciting situations by training your nervous system to tolerate intense arousal without reflexively ejaculating. That's what progressive exposure training accomplishes.
Frequency of Sexual Activity
The interval between sexual activities influences sensitivity profoundly. After long abstinence—say, a week or more—seminal accumulation and increased excitatory neurotransmitters reduce control. Your body has been primed, loaded, ready to fire at the slightest provocation.
It's like filling a water balloon beyond capacity: the slightest touch makes it burst.
Conversely, overly frequent activity can cause fatigue and irritability that also lower endurance. Your pelvic floor muscles become overworked, your neurotransmitter balance shifts, and performance suffers.
A balanced sexual rhythm—neither abstinent nor compulsive—supports optimal regulation. For most men, this means regular sexual activity (2-4 times weekly) with occasional variation. Your body learns predictable patterns, maintains healthy neurotransmitter balance, and avoids both the hair-trigger sensitivity of prolonged abstinence and the fatigue of excessive frequency.
Age and Lifestyle Factors
How Age Affects Ejaculatory Control
Picture your nervous system as a complex network of wires. In younger men, these wires conduct signals at lightning speed—nerve impulses race from stimulus to reflex in milliseconds. Testosterone surges, sensitivity peaks, and the ejaculatory reflex fires fast.
Age alters this equation in complex ways.
Neural conduction velocity naturally slows slightly with age. The lightning-fast reflexes of youth gradually moderate. Testosterone levels decline about 1-2% annually after age 30, which can reduce the hair-trigger sensitivity many younger men experience.
For some men, this creates a paradox: control actually improves with age as the nervous system becomes less hyperresponsive. The 22-year-old who struggled to last two minutes may find that at 42, five to seven minutes comes naturally—without any conscious training.
However, age also introduces new challenges. Conditions like prostatitis (prostate inflammation), diabetes (which damages nerves), and vascular issues (affecting blood flow) become more common. These can reverse the natural advantage of age, causing PE to emerge or worsen in men who previously had good control.
The key insight: age isn't destiny in either direction. Young men can develop excellent control through training. Older men can maintain or improve control by addressing underlying health conditions and practicing the techniques that work at any age.
Sleep, Exercise, and Diet Impact
Your body is an interconnected system. When one component suffers, everything else pays the price.
Sleep deprivation raises cortisol (stress hormone) and decreases testosterone (power hormone)—a double hit against ejaculatory control. Men who consistently sleep fewer than six hours report significantly worse sexual performance and shorter latency times. Your nervous system needs quality rest to maintain the delicate neurotransmitter balance required for control.
Exercise—especially aerobic activity—improves serotonin signaling (your natural brake) and pelvic circulation. Studies show men with regular physical activity suffer less from PE than sedentary counterparts. A 30-minute run triggers neurochemical changes that persist for hours, improving your control window later that evening.
Diet matters more than most men realize. Foods rich in omega-3 fatty acids (fish, flaxseed) support neurotransmitter synthesis. Magnesium (nuts, spinach, dark chocolate) regulates nervous system excitability. Tryptophan (turkey, eggs, cheese) converts to serotonin—your ejaculatory brake pedal.
Conversely, high-sugar diets and processed foods promote metabolic inflammation and reduce serotonin synthesis. Energy drinks and excessive caffeine overstimulate your sympathetic nervous system, making control harder.
Think of lifestyle factors as the foundation of a house. You can have the best furniture and decorations (techniques), but if the foundation (sleep, exercise, nutrition) is crumbling, nothing stays stable.
Alcohol, Drugs, and Medications
The relationship between substances and ejaculatory control is complex and often counterintuitive.
Alcohol in small amounts may initially seem to delay ejaculation by slightly numbing sensations. But this is deceptive: chronic use desensitizes dopamine receptors, eventually worsening control. Heavy drinkers often develop erectile dysfunction and premature ejaculation—the worst of both worlds.
SSRIs (antidepressants like sertraline, fluoxetine, paroxetine) deliberately increase serotonin to delay ejaculation. They're sometimes prescribed specifically for PE treatment. But they come with side effects: decreased libido, emotional blunting, potential dependency. Still, for some men, short-term pharmaceutical support while learning behavioral techniques makes sense.
Recreational stimulants (cocaine, amphetamines) have the opposite effect—they heighten sympathetic activity dramatically, often causing faster ejaculation despite the user feeling more aroused and confident. The neurochemical reality contradicts the subjective experience.
Cannabis shows mixed effects: some men report better control due to anxiety reduction and altered time perception; others find it increases sensitivity and shortens latency. Individual reactions vary widely.
Always review medications with a physician if PE appears after starting a new drug. Many prescription medications (certain blood pressure meds, ADHD stimulants, etc.) affect sexual function as side effects.
→ Lifestyle creates the foundation, but specific training builds the structure. You need both. The Complete 4-Level Program addresses lifestyle optimization and systematic neural retraining—because lasting control requires both elements working in harmony.
When to See a Doctor
Primary vs. Secondary Premature Ejaculation
Medical professionals distinguish between two distinct patterns:
Primary (lifelong) PE has been present since your first sexual experiences. You've never known anything different. Every partner, every situation—the pattern remains consistent. This form often reflects neurochemical predispositions: your serotonin system may be less sensitive, your reflex arc more excitable, your pelvic floor naturally hypertonic.
Secondary (acquired) PE develops later after a period of normal function. You used to last 8-10 minutes comfortably, but over the past year, it's dropped to 2-3 minutes. This sudden change typically signals an underlying medical condition, psychological stressor, or relationship issue.
The distinction matters because treatment approaches differ:
- Primary PE usually responds well to behavioral training combined with lifestyle modifications, though some men benefit from short-term SSRI support during the learning phase.
- Secondary PE requires identifying and addressing the root cause: Is it a new medication? Prostate inflammation? Relationship stress? Once the trigger is resolved, control often returns naturally.
If you're unsure which category fits you, tracking patterns helps: When did this start? Has it always been this way, or is it recent? Does it happen with all partners or specific situations?
Medical Conditions to Rule Out
Before assuming your PE is purely behavioral or psychological, certain medical conditions should be ruled out:
Prostatitis or urethritis (inflammation of prostate or urethra) creates hypersensitivity that shortens latency. Pain, burning during urination, or discomfort in the pelvic region are warning signs. Treatment with antibiotics or anti-inflammatories often resolves both the inflammation and the PE.
Thyroid dysfunction, particularly hyperthyroidism, directly affects ejaculatory timing. When your thyroid produces excess hormone, it speeds up everything—heart rate, metabolism, reflexes, including sexual reflexes. A simple blood test can detect this. Correcting thyroid levels typically eliminates PE completely.
Neurological disorders affecting the spinal cord or peripheral nerves can alter reflex pathways. Multiple sclerosis, spinal cord injuries, or severe diabetic neuropathy may present with ejaculatory dysfunction. If you have other neurological symptoms (numbness, weakness, coordination issues), this warrants investigation.
Diabetes and insulin resistance damage both nerves and blood vessels over time, affecting sexual function in multiple ways. Some diabetic men experience PE; others develop delayed ejaculation or erectile dysfunction. Managing blood sugar through diet, exercise, and medication protects sexual function.
Penile hypersensitivity syndromes sometimes result from scarring, inflammation, or congenital variation. If your glans is exquisitely sensitive—painful even with light touch—specialized desensitization therapy or consultation with a urologist may help.
A clinical evaluation typically includes:
- Complete medical history
- Physical examination (checking for prostate tenderness, penile abnormalities)
- Blood tests (thyroid function, testosterone, prolactin, glucose)
- Urinalysis (ruling out infection)
Red flags that require immediate medical consultation:
- Painful ejaculation or erection
- Blood in semen or urine
- Sudden erectile dysfunction combined with PE
- Unexplained weight loss, fever, or night sweats
- History of pelvic surgery or trauma
- PE that develops suddenly after age 50
Don't self-diagnose. A skilled urologist or men's health specialist can identify treatable medical causes in minutes—causes that behavioral training alone won't fix.
Treatment Options Overview
Understanding the cause guides treatment. Here's how different causes map to solutions:
Physical causes → Physical interventions:
- Penile hypersensitivity: Sensory retraining, graduated exposure, topical desensitizers (short-term)
- Pelvic floor dysfunction: Physiotherapy, Kegel training, reverse Kegels, biofeedback
- Hormonal imbalances: Medical correction (thyroid medication, targeted SSRI therapy)
Psychological causes → Psychological interventions:
- Performance anxiety: Cognitive-behavioral therapy (CBT), anxiety management techniques
- Stress/trauma: Mindfulness training, stress reduction protocols, sometimes therapy
- Conditioned reflexes: Stop-start method, squeeze technique, progressive desensitization
Lifestyle factors → Lifestyle modifications:
- Poor sleep: Sleep hygiene optimization, sleep disorder treatment
- Sedentary lifestyle: Regular aerobic and pelvic floor exercise
- Substance use: Reduction or elimination of alcohol/drugs affecting control
Relational factors → Couples work:
- Partner dynamics: Communication training, sensate focus exercises
- Anxiety cycles: Joint therapy, collaborative technique practice
The most effective approach? Comprehensive, integrating multiple elements. A man with lifelong PE might combine:
1. Daily Kegel exercises (physical)
2. Stop-start training 3x/week (behavioral reconditioning)
3. Mindfulness meditation 10 min/day (stress management)
4. Partner communication sessions weekly (relational)
5. Short-term SSRI if needed (pharmaceutical support during learning)
This multi-modal approach addresses the problem from every angle, creating robust, lasting change.
→ The Complete 4-Level Ejaculation Mastery Program is specifically designed as this comprehensive, multi-modal solution. It combines physical training (Kegels, reverse Kegels), behavioral reconditioning (stop-start, squeeze), psychological tools (breathing, mindfulness), and relational strategies (partner communication)—all structured in a progressive system that takes you from 0% to 100% mastery step by step.
How Understanding Causes Helps Treatment
Targeted Solutions Based on Root Cause
Imagine trying to fix a car without knowing what's wrong. You might replace the battery when the real problem is the alternator. You waste time, money, and frustration on solutions that can't possibly work—because you're addressing the wrong cause. The same applies to premature ejaculation. When you understand why it happens, you stop applying random tips and start using cause-specific interventions.
If hypersensitivity dominates → Sensory retraining:
- Graduated exposure exercises
- Mindful attention training
- Strategic position selection (less stimulating angles)
- Temporary desensitization aids while learning control
If anxiety dominates → Autonomic regulation:
- Diaphragmatic breathing (activates parasympathetic system)
- Progressive muscle relaxation
- Cognitive restructuring (changing anxiety-producing thoughts)
- Exposure therapy (gradually increasing comfort in intimate situations)
If hormonal imbalance drives it → Medical optimization:
- Thyroid correction for hyperthyroidism
- Short-term SSRI therapy to boost serotonin
- Testosterone management if levels are problematic
- Treatment of underlying conditions (prostatitis, diabetes)
If conditioning is the culprit → Neural reprogramming:
- Stop-start method (the gold standard)
- Squeeze technique
- Edging practice
- Mindful masturbation to rewrite old patterns
If pelvic floor dysfunction exists → Neuromuscular retraining:
- Standard Kegels (strengthening)
- Reverse Kegels (relaxation—often the missing piece)
- Biofeedback training
- Physical therapy for hypertonic pelvic floor
If relationship dynamics contribute → Couples work:
- Communication skills training
- Sensate focus exercises (taking pressure off performance)
- Collaborative technique practice
- Rebuilding trust and reducing judgment
This precision approach yields lasting control, not temporary delay. You're not just masking symptoms—you're correcting underlying dysfunction.
Most men discover their PE has multiple contributing causes. Perhaps it started with performance anxiety (psychological), which created chronic tension (physical), which shortened your fuse, which increased anxiety further (vicious cycle). Breaking this requires addressing all components simultaneously.
Why Generic Advice Fails
"Just think about baseball." "Try a second round." "Use thick condoms." "Masturbate before sex." You've heard the advice. Maybe you've tried it. And you've discovered what millions of men know: generic tips rarely work for long, if at all.
Why? Because they're not tailored to your specific causes. They're band-aids on bullet wounds.
The "think about something else" approach tries to reduce arousal by distraction. But if your problem is a hyperactive reflex arc or low serotonin, mental distraction can't override neurophysiology. You might gain 30 seconds—before biology reasserts control.
The "second round" strategy assumes your refractory period will give you more endurance. For some men, this works temporarily. But it doesn't teach control, it just exploits temporary desensitization. And it requires ejaculating first—which may not fit your partner's needs or your own goals.
Thick condoms or desensitizing sprays reduce sensation. They might help if hypersensitivity is your primary issue. But if anxiety or pelvic floor dysfunction drives your PE, numbing yourself solves nothing. You're just adding numbness to the existing problem.
Pre-sex masturbation depletes your "first shot" so the second lasts longer. But this is exhausting, time-consuming, and still doesn't build actual control. You're managing symptoms, not developing skill.
What works? Systematic, cause-specific training that addresses your unique combination of factors. This requires:
1. Understanding your specific causes (physical? psychological? hormonal?)
2. Selecting appropriate interventions for those causes
3. Practicing consistently with progressive difficulty
4. Tracking results and adjusting based on what works
5. Building real, transferable skill—not temporary workarounds
The difference between generic advice and targeted training is the difference between hoping for a lucky break and systematically building competence.
Why a Complete System Works Best
Premature ejaculation is multifactorial. Addressing just one cause while ignoring others is like trying to fix a three-legged stool by repairing only one leg. The system remains unstable.
True mastery requires integration:
Physical foundation: Strong, responsive pelvic floor muscles that can contract (to delay ejaculation) and relax (to reduce tension). This comes from progressive Kegel training and reverse Kegels—not just generic "squeeze and hold" exercises.
Neurological rebalancing: Shifting from sympathetic dominance (stress, fight-or-flight) to balanced autonomic tone. This requires breathwork, mindfulness, and stress management—techniques that literally change your brain's activity patterns.
Behavioral reconditioning: Unlearning rush-to-orgasm patterns and installing new neural pathways that tolerate high arousal without reflexive ejaculation. This demands structured practice: stop-start, squeeze technique, edging—progressing from solo practice to partnered sex.
Psychological resilience: Breaking the performance anxiety cycle by building confidence through small wins, cognitive restructuring, and exposure therapy. You can't think your way out of PE, but you can't succeed without addressing the mental component either.
Relational harmony: Creating a supportive dynamic where your partner becomes an ally, not a source of additional pressure. This involves communication training, sensate focus, and collaborative problem-solving.
Lifestyle optimization: Sleep, exercise, nutrition, and stress management form the foundation on which everything else rests. Neglect these, and even perfect technique struggles against biological headwinds.
Only a structured, step-by-step system addressing all six components creates permanent results. Anything less is incomplete.
Introducing the 4-Level Mastery System
Imagine having a clear roadmap where you know exactly what to practice each day, how to measure progress, and when you're ready to advance. No guessing, no conflicting advice, no wasted effort.
That's what a progressive system provides.
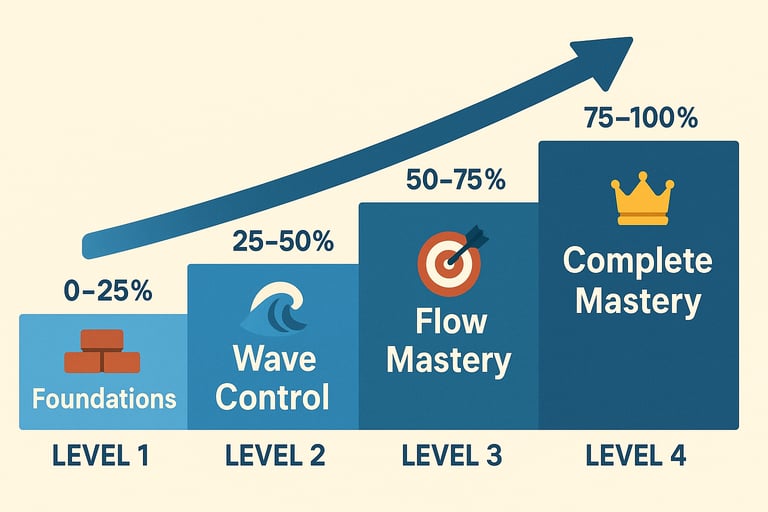
The Complete 4-Level Scientific System for Ejaculatory Mastery guides you through:
Level 0-25%: Foundations
- Locating and activating your pelvic floor muscles
- Basic Kegel exercises (standard and reverse)
- Understanding the 0-10 arousal scale
- First successful stops in solo practice
- Establishing baseline measurements
Level 25-50%: Wave Control
- Stop-start mastery across multiple cycles
- Squeeze technique for emergency control
- "Elevator" Kegels for fine-tuned control
- Breathing and arousal regulation
- Introducing partner exercises (non-penetrative)
Level 50-75%: Flow Mastery
- Full penetration control techniques
- Advanced pacing (rhythm, depth, pressure variations)
- Micro-pauses and positional strategies
- Attentional anchoring during high arousal
- Multiple stop-start cycles during intercourse
Level 75-100%: Complete MasteryThe 4-Level Training Program
- Conscious choice of ejaculation timing
- Robustness in challenging contexts (stress, novelty, abstinence)
- Automatic application of techniques without conscious thought
- Integration of all skills into natural sexual expression
Beyond 100%: Advanced Techniques
- Multiple male orgasms (orgasm without ejaculation)
- Tantric energy circulation
- Full-body orgasmic experiences
- Sexual energy transmutation
This isn't theory. It's not wishful thinking. It's a proven, systematic approach used by over 10,000 men worldwide, backed by 50+ clinical studies in sexual medicine, and structured around the same principles used in neurological rehabilitation and behavioral therapy.
You don't need to figure this out alone. You don't need to waste years experimenting with random techniques. You need a clear path from where you are now to complete mastery—and that's exactly what this system provides.
→ Ready to stop guessing and start mastering? Access the Complete 4-Level Program here and begin your transformation today.
Frequently Asked Questions
Is premature ejaculation purely psychological?
No—but psychology plays a role.
The idea that PE is "all in your head" is a myth that causes unnecessary shame. Research clearly shows that biological and neurochemical factors often set the foundation. Men with naturally low serotonin receptor sensitivity have a physiological disadvantage before psychological factors even enter the picture.
That said, psychology matters immensely. Performance anxiety creates physiological changes (elevated cortisol, sympathetic activation, increased nerve sensitivity) that accelerate the reflex. It's a mind-body interaction, not one or the other.
Think of it this way: biology loads the gun, psychology pulls the trigger. Both must be addressed for lasting control.
Can hormones really cause premature ejaculation?
Absolutely—and this is well-documented in clinical studies.
Low serotonin levels increase ejaculatory reflex excitability. This isn't speculative—it's the mechanism behind why SSRIs (which boost serotonin) are prescribed for PE treatment.
Thyroid imbalances, particularly hyperthyroidism, directly accelerate ejaculation. Multiple studies show that correcting thyroid dysfunction resolves PE in many cases without any other intervention.
High testosterone can increase libido and sensitivity, potentially shortening latency in some men—though the relationship is complex and individual.
Other hormones (prolactin, oxytocin) affect refractory periods and satisfaction. The hormonal orchestra must play in harmony for optimal sexual function.
If your PE appeared suddenly without clear psychological or situational triggers, hormonal screening is essential. A simple blood test can reveal correctable imbalances.
Does masturbation frequency affect control?
Yes, but the relationship is nuanced.
Rushed masturbation conditions your nervous system for rapid orgasm. If you spent your teenage years quickly masturbating before someone walked in, you trained a "sprint to orgasm" reflex. This pattern persists into partnered sex until consciously retrained.
Excessive masturbation (multiple times daily) can desensitize dopamine receptors and fatigue pelvic floor muscles, potentially worsening control.
Complete abstinence creates hypersensitivity. After a week without release, seminal buildup and heightened excitatory signals shorten your fuse dramatically.
Mindful, measured masturbation serves as excellent training ground. Using stop-start techniques, practicing arousal awareness, and deliberately extending duration teaches your nervous system the control patterns you want.
The key isn't frequency—it's how you masturbate. Rushed, mechanical self-stimulation reinforces the problem. Conscious, patient practice builds the solution.
Are there medications that help?
Yes—several pharmaceutical options exist, each with specific use cases:
SSRIs (Selective Serotonin Reuptake Inhibitors) like paroxetine, sertraline, and fluoxetine increase serotonin levels, which delays ejaculation. These are prescribed either daily (building up serotonin over weeks) or on-demand a few hours before sex.
- Pros: Effective for many men, well-studied, FDA-approved for other uses
- Cons: Side effects (decreased libido, emotional blunting), don't teach actual control, require ongoing use
Dapoxetine is a short-acting SSRI specifically designed for PE, taken 1-3 hours before sex.
- Pros: Shorter half-life reduces side effects, designed specifically for PE
- Cons: Not available in all countries (including the US), still has SSRI side effects
Topical anesthetics (lidocaine, prilocaine creams or sprays) numb penile sensitivity temporarily.
- Pros: Work immediately, no systemic side effects, available over-the-counter
- Cons: Can numb partner, reduce your own pleasure, don't build lasting control
Tramadol (an opioid pain medication) has ejaculation delay as a side effect and is sometimes prescribed off-label.
- Cons: Addiction potential, significant side effects, not FDA-approved for PE
PDE5 inhibitors (Viagra, Cialis) primarily treat erectile dysfunction but can help some men with PE—particularly if anxiety about erection quality contributes to rushing.
The crucial point: Medications can provide temporary relief or support during the learning phase, but they don't teach your nervous system new patterns. The most successful approach combines short-term pharmaceutical support with behavioral training—then maintains results through skill alone.
Can pelvic floor exercises fix PE?
They can significantly help—especially when combined with other techniques.
Research shows that pelvic floor physiotherapy produces meaningful improvements in ejaculatory latency for many men. The combination of strengthening exercises (standard Kegels) and relaxation training (reverse Kegels) addresses both hypertonicity and weakness.
Why they work:
1. Strengthening gives you the ability to actively contract and temporarily delay the reflex
2. Relaxation training reduces chronic tension that accelerates ejaculation
3. Neuromuscular awareness helps you consciously modulate arousal
4. Improved blood flow supports erectile quality and endurance
But Kegels alone aren't enough. They're one component of a comprehensive system. Men who only do Kegels without addressing breathing, anxiety, or behavioral patterns see limited results.
Think of Kegels as building the muscle. You still need to learn how to use that muscle strategically—which requires training in actual sexual contexts (stop-start, squeeze, arousal modulation).
The men who succeed combine strong pelvic floor muscles with breathwork, mindfulness, and progressive behavioral exposure. That's why integrated programs outperform single-technique approaches.
When should I consult a professional?
Seek medical consultation if:
- PE causes significant personal distress or relationship problems
- Ejaculation occurs before or immediately upon penetration (severe PE)
- You experience painful ejaculation or erection
- PE appeared suddenly after a period of normal function (secondary PE)
- You have other symptoms (pain, blood in semen, urinary issues)
- You're over 50 and PE just started (rule out prostate issues)
- Self-help techniques haven't improved things after 3 months of consistent practice
See a urologist or men's health specialist for:
- Medical evaluation (ruling out prostatitis, thyroid issues, neurological problems)
- Hormonal testing if indicated
- Discussion of pharmaceutical options
- Severe cases requiring specialized intervention
Consider sex therapy or counseling if:
- Performance anxiety is severe and pervasive
- Relationship issues significantly contribute
- Past trauma affects sexual function
- You need guided support through behavioral techniques
The good news: The majority of men with PE can achieve significant improvement through structured self-directed training. Professional consultation is important for ruling out medical causes and getting personalized guidance—but the actual work of building control happens through consistent practice, which you can do independently with the right system.
Conclusion: From Understanding to Action
You now understand premature ejaculation from every angle: the spinal reflexes and neurotransmitters, the pelvic floor and hormones, the psychology and relationships, the lifestyle factors and medical conditions. You've seen how each cause points to specific solutions, and why comprehensive, integrated approaches outperform quick fixes.
But understanding alone doesn't create change. Knowledge without application remains theoretical. The gap between knowing what works and actually doing it determines whether you stay stuck or break through.
The men who succeed share three characteristics:
1. They commit to systematic practice rather than hoping for magic bullets
2. They track progress objectively instead of relying on feelings alone
3. They follow a proven structure rather than improvising randomly
Premature ejaculation isn't a character flaw, a permanent condition, or evidence of inadequacy. It's a trainable skill deficit—and like any skill, it improves through deliberate practice with the right methodology.
The pathway from where you are now to complete mastery is clear:
Understand your causes → Identify which factors most affect you
Select appropriate techniques → Focus on interventions that address your specific causes
Practice systematically → Follow a progressive structure from simple to advanced
Track and adjust → Measure results, refine approach based on what works
Build lasting competence → Transform conscious effort into automatic skill
This isn't about perfection. It's about progress. Every man who achieved lasting control started exactly where you are now—frustrated, perhaps discouraged, but ready for something better.
The question isn't whether you can develop ejaculatory mastery. The research confirms you can. The question is whether you'll take the first step.
Your Next Step
Thousands of men have transformed their sexual confidence using the evidence-based system we've referenced throughout this guide. They started with uncertainty and built unshakeable control through progressive, scientific training.
The Complete 4-Level Ejaculation Mastery Program gives you:
✓ Clear progression from 0% to 100% mastery
✓ Daily practice protocols so you always know what to do
✓ Objective measurements to track your improvement
✓ Solo and partner exercises for real-world application
✓ Advanced techniques (multiple orgasms, tantric practices) once basics are mastered
✓ Lifetime access to continue refining your skills
Based on 50+ peer-reviewed studies and used successfully by over 10,000 men worldwide, this system doesn't guess—it systematically rebuilds your ejaculatory control from the neurological foundation up.
Stop hoping for change. Start creating it
→ Access the Complete 4-Level Ejaculation Mastery Program. Your transformation begins the moment you decide it does. Why wait another day?
Medical Disclaimer: This content is for educational purposes and doesn't replace professional medical advice. Consult a healthcare provider for personalized diagnosis and treatment, especially if you experience pain, sudden changes in sexual function, or symptoms suggesting underlying medical conditions.
→ Understanding these situational factors helps you predict challenges. The Complete Mastery System includes specific strategies for managing high-novelty situations, partner dynamics, and frequency variations—so you maintain control in every context, not just ideal conditions.



A guide to male sexual confidence and happiness
Guide for educational purposes. Consult a healthcare professional for persistent problems.
© 2025. All rights reserved.
🔒 Secure Checkout
📱 Instant Download
💳 PayPal & Credit Cards Accepted with
🤫 Discreet payment receipt